Being a doctor
Medicine is a lonely business. Few can help you to make a diagnosis. No one is available if there is a misdiagnosis. It is an opportunity inside a risk. What is needed is initiative, knowledge, skill, courage, and perseverance. The reward is intuition and prescience. Always do the impossibly difficult job.
We do not have to better than anyone. We just need to be better than ourselves everyday.
Medicine is a lonely business. Few can help you to make a diagnosis. No one is available if there is a misdiagnosis. It is an opportunity inside a risk. What is needed is initiative, knowledge, skill, courage, and perseverance. The reward is intuition and prescience. Always do the impossibly difficult job.
We do not have to better than anyone. We just need to be better than ourselves everyday.
solve cases and earn CREDIT*
Try these cases, they are not designed to trick you. These were real cases. Patients do not come in with their diagnosis. The provider decides what is dangerous or not and who needs treatment, an injection or not. Are you ready to back up your plan with your thought and your documentation? If you have interesting cases to share, send it to us and earn Honorarium here.
Please review the following cases and provide a working differential diagnosis and a map to workup. You could earn $25 credit per solved case toward your live CME registration fee (up to $100 per CME per attendee)*.
Please review the following cases and provide a working differential diagnosis and a map to workup. You could earn $25 credit per solved case toward your live CME registration fee (up to $100 per CME per attendee)*.
Case 119 Sciatica

35 year old man with severe left sciatica and had to have back surgery done. But the pain never improved and he was forced to retire prematurely. He was on Morphine for years. He came for a second opinion. He had severe pain in the middle of his left buttock down his left leg reproducing his left leg pain. What could be an alternative diagnosis and treatment plan than surgery. Please provide ICD code and CPT code if you can.
CAse 120 Chest pain

16 year old boy new, sudden onset, sharp, progressive right chest pain with progressive dyspnea. His trachea was deviated to the left side. Vocal resonance and chest expansion were reduced on right chest auscultation. What was the diagnosis and plan. Describe your approach. reference withheld.
Case 121 BAck and leg pain

57 year old man with history of hypertension, hyperlipidemia, morbid obesity and diabetes, presented to ED for sudden onset middle to low back pain with severe shooting right leg pain. The pain is tearing in nature and the patient could not move his right leg nor walk. He was given pain killers which helped the pain. Xray of the hip and L-spine were done. These showed lumbar DDD. The ED doctor diagnosed with sciatica. He was reminded to follow up his PMD and discharged from ED. The pain never resolved and the next day, he presented to another ED for the same pain. What would your differential diagnosis and plan. Outcome and ref withheld.
Case 122 Chest pain

|

|
This is a very old case- more than 100 years old. The knowledge is not.
38 year old man with dull right chest pain that radiates back to his right shoulder blade area. He has frequent brassy cough that can be dry at times and very wet and productive with purulent mucus the next. His voice is hoarse. He also has a mild dyspnea. Outcome and ref withheld.
38 year old man with dull right chest pain that radiates back to his right shoulder blade area. He has frequent brassy cough that can be dry at times and very wet and productive with purulent mucus the next. His voice is hoarse. He also has a mild dyspnea. Outcome and ref withheld.
Case 123 clumsy child

7 year old right handed girl (handiness achieved around 1 year of age), product of an uncomplicated pregnancy and delivery of non-consanguineous parents, achieved all major developmental milestones in height, weight, speech and languages, intelligence and dexterity (competes in math and piano), has an unresolved left hip and leg clumsiness since she started walking around 12 months of age. She has been to many pediatric specialists over the years. She was referred to an orthopedic surgeon when her family relocated to another state. Spine, pelvis, hip and knee and leg Xray were done and they were all normal. Bone and joint integrity and range of motion were all normal. The surgeon then refer her to a pain doctor. On further examination, the child was normal in appearance, age and interaction, pleasant and cheerful. She fully and ably cooperates with examination. UE and gait were normal. The one abnormal findings were she favored right leg to walk, to climb, and to bear weight. Her left leg was ever so slightly thinner than right. There was slight medial rotation of left leg and slight left toe walking. She could jump on both legs or right leg but not on her left leg nor could she stand on her left leg by herself. She had good insight about her deficit as she stated clearly to her doctor- "I can not do that!". Yet there was no pain when she stands on her left leg with help. What additional history and physical examination could be done and how could these help determine this girl's favoritism of her right leg and plan of action. Thank you.
CASE 124 CHEST PAIN

|

|
47 year old man with 20 year history of left side chest pain. The pain of achy and squeezing quality. He felt the pain at times to his left chin, neck, shoulder and left arm and forearm. The pain usually happened with cooler weather and lasted for 1 minute and could recur several times a days over days. The pain was self-limited.
It could be triggered by leaning on his left arm and shoulder. Exercise, even intense one, did not trigger his pain. Ibuprofen reliably stopped the pain until its recurrence 6 to 12 months later.
He could partially reproduce the pain by pushing hard over left chest bone and rib cage junction area, indicated with red star. These pain along sternum sometimes happens on the right side. He had no other pain/symptoms/signs.
It could be triggered by leaning on his left arm and shoulder. Exercise, even intense one, did not trigger his pain. Ibuprofen reliably stopped the pain until its recurrence 6 to 12 months later.
He could partially reproduce the pain by pushing hard over left chest bone and rib cage junction area, indicated with red star. These pain along sternum sometimes happens on the right side. He had no other pain/symptoms/signs.
CASE 125 CHEST PAIN

32 year old man started training for a half marathon and developed a bilateral lower chest pain.
Running with rapid and deeper breathing worsened the pain. Grabbing onto a horizontal bar and doing pull-ups worsened the pain. Resting and slower breathing eased the pain. There was no tenderness over chest and abdomen. He noticed the pain was getting better with warming up and gradual acclimation to the vigor of exercise.
He was healthy otherwise.
Running with rapid and deeper breathing worsened the pain. Grabbing onto a horizontal bar and doing pull-ups worsened the pain. Resting and slower breathing eased the pain. There was no tenderness over chest and abdomen. He noticed the pain was getting better with warming up and gradual acclimation to the vigor of exercise.
He was healthy otherwise.
CASE 126 "Pulling" PAIN in abdomen, back, and leg

|

|
61 year old man with long standing lightening strike pain for both legs pulling from his feet. He recently develop a new pulling pain deep in his pelvis all the way up to his left upper abdomen. On examination, he has has deficit of deep joint sensation. What could be this pain and its cause. Referrene withheld.
CASE 127 abdominal PAIN

57 year old man with 5 year history of constant mild abdominal pain much severe after ingestion of food or water. The symptoms are progressively worse over time He has anorexia and cachexia due to his inability to eat. PMH includes insulin dependent Type 2 Diabetes x 15 years, heavy smoker x decades, DB related neuropathy, retinopathy and nephropathy. PE: diffused abdominal pain with deep tenderness overall but nonfocal. Labs showed no DKA and HbA1c was 7.1%. What could be the differential diagnosis. Reference withheld.
CASE 128 Hand PAIN and tingling

Please name this lesion.
CASE 129 headache
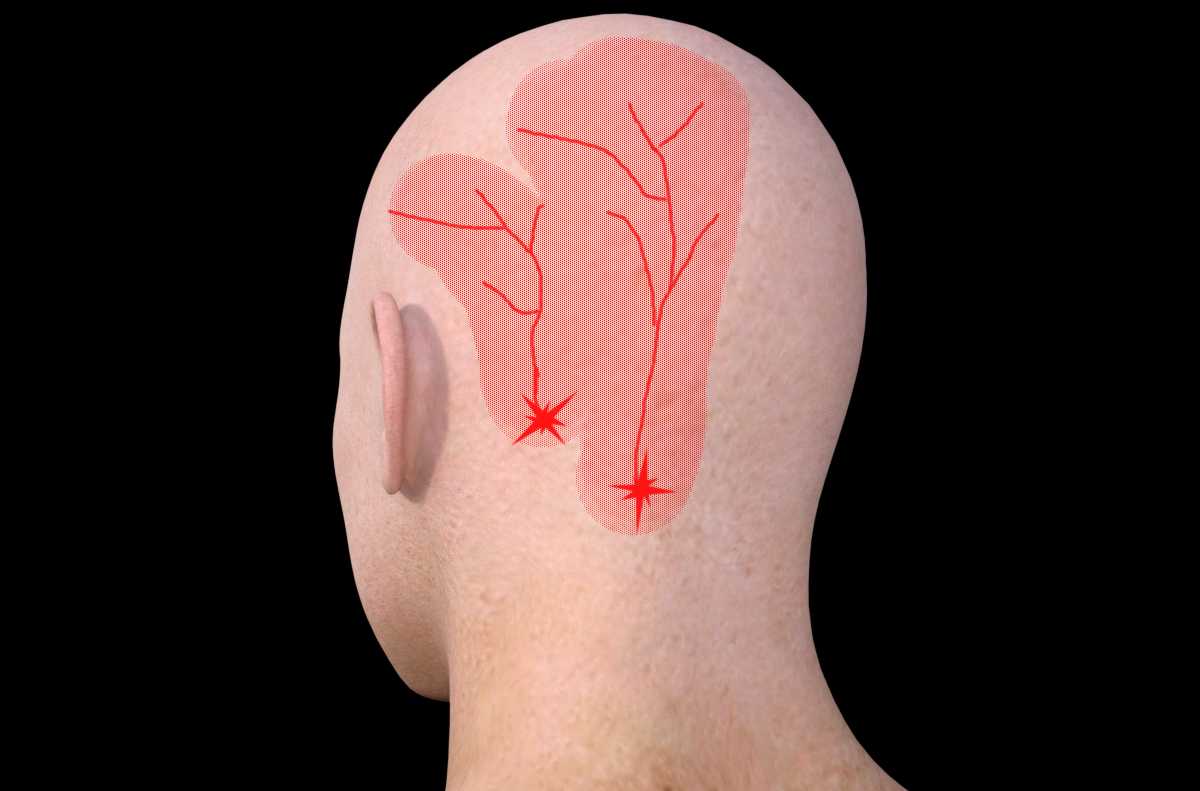
Please name this type of headache and neck pain. Please provide treatment and injection options and their CPT codes/ICD-10 codes.
CASE 130 face or jaw PAIN

|

|
45 year old man with 3 year history of right face pain. He has been to many dentists and oral surgery. What is the cause of his pain and how it should be treated. Please provide CPT codes/ICD-10 codes.
* Once submitted, upon review and approval, you will receive $25 credit per case toward any CME live program within 36 months. Credit has no cash value but can be redeemed at registration of CME via an issued coupon. There is NO limit of credit earned. It is non-transferable to other providers. It can be combined with other credit but no more than $100 can be used toward any single live CME per person.